

Cyclospora treatment requires a specific prescription antibiotic, and knowing which one matters, because not all GI infections respond to the same medications. With a confirmed cyclosporiasis outbreak underway in Southeast Michigan in 2026, providers and patients alike need to understand the correct diagnostic and treatment approach. This post covers how Cyclospora is tested, the recommended antibiotic regimen, what recovery looks like, and what to do if you have a sulfa allergy.
For background on the outbreak and symptom information, see our posts on the Michigan Cyclospora outbreak 2026 and cyclospora symptoms.
Technically, the human immune system can eventually clear Cyclospora without antibiotics. However, the illness may take a month or longer to resolve without treatment, and symptoms often follow a relapsing course: improving briefly before returning. The fatigue associated with cyclosporiasis can also persist beyond the resolution of diarrhea, affecting daily function for weeks.
For most patients, waiting it out is not a practical or comfortable strategy. Antibiotic treatment dramatically shortens the illness and significantly reduces the chance of relapse. If you have had symptoms for more than a few days, seeking treatment is the appropriate course of action.
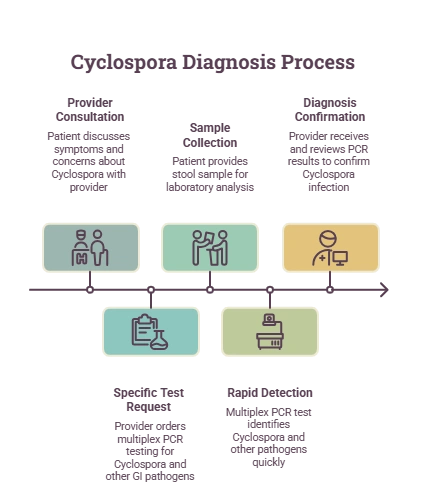
A provider must confirm Cyclospora infection before prescribing antibiotic treatment, and the right test must be requested. This is a critical detail: standard stool ova and parasite (O&P) testing does not automatically screen for Cyclospora. The parasite requires specific staining techniques and must be explicitly listed on the lab order.
The preferred test at this time is multiplex PCR testing, such as the BioFire GI panel. This test:
When you visit a provider, be specific: tell them you are concerned about Cyclospora given the current Michigan outbreak, that your symptoms have lasted more than a few days, and whether they have relapsed. This helps ensure the correct test is ordered. MI Express Urgent & Primary Care providers are equipped to order GI stool testing at your visit, including send-out options for PCR panels.
For a sense of the in-house testing capabilities at MI Express Urgent & Primary Care, our rapid strep testing page gives an example of how we handle time-sensitive infectious illness testing on-site.
The only antibiotic recommended for cyclosporiasis is trimethoprim-sulfamethoxazole (TMP-SMX). You may recognize it under its brand names: Bactrim, Septra, or Cotrim. This is a sulfa-class antibiotic.
Standard treatment course: TMP-SMX taken twice daily for 10 days. Symptoms typically begin to improve within a few days of starting the antibiotic. Completing the full 10-day course is important, even if you feel better earlier, to ensure the parasite is fully cleared.
The CDC clinical guidance for cyclosporiasis confirms TMP-SMX as the preferred treatment. No alternative antibiotic has demonstrated equivalent efficacy for cyclosporiasis in clinical data.
This is an important and common question. If you have a documented allergy to sulfa drugs, TMP-SMX cannot be used safely. In this situation, discuss your allergy with your provider before treatment begins.
Some providers have used ciprofloxacin as an alternative, though clinical evidence for its efficacy against Cyclospora is limited compared to TMP-SMX. Your provider will weigh your allergy history and symptom severity to determine the most appropriate course of action. Do not take TMP-SMX if you have a sulfa allergy without explicit guidance from a provider.
With antibiotic treatment, most patients begin to notice improvement within two to three days. Diarrhea frequency and abdominal cramping typically reduce first, with fatigue and appetite returning over the following week. Completing the full 10-day course of TMP-SMX is important, even when you feel significantly better, to prevent incomplete clearance and recurrence.
Staying well-hydrated throughout the illness and recovery period is essential. Cyclospora-associated diarrhea can lead to dehydration, particularly in older adults, young children, and anyone with a health condition that reduces fluid reserves. If you are struggling to stay hydrated, a provider can assess whether IV fluids are needed.
Completing the full antibiotic course substantially reduces the risk of recurrence. However, reinfection is possible if you are re-exposed to contaminated food or water after recovery. There is no immunity acquired from a previous Cyclospora infection. During the current outbreak period, continuing to wash all fresh produce thoroughly and avoiding raw produce from unknown sources remains prudent.
For most otherwise healthy adults, urgent care is entirely appropriate for Cyclospora evaluation and treatment. A provider can order the correct stool test, review your symptoms, rule out other GI conditions, and write the prescription. You do not need a referral to a gastroenterologist for an uncomplicated case of cyclosporiasis.
If you are immunocompromised, pregnant, elderly, or experiencing severe dehydration, a higher level of care may be appropriate. In those situations, your urgent care provider will advise you accordingly.
Most patients notice improvement in diarrhea and cramping within two to three days of starting TMP-SMX. Completing the full 10-day antibiotic course is important to prevent recurrence of symptoms.
Yes. TMP-SMX, the only recommended antibiotic for cyclosporiasis, requires a prescription. Over-the-counter antidiarrheal medications may reduce symptoms temporarily but will not eliminate the parasite.
Over-the-counter antidiarrheal products may provide temporary symptom relief but do not treat the underlying infection. Antibiotic treatment with TMP-SMX is required to clear the parasite and prevent relapse.
Untreated cyclosporiasis typically persists for weeks to a month or longer, often with a relapsing pattern. Prolonged illness can lead to dehydration, weight loss, and extended fatigue affecting daily activities.
TMP-SMX has specific safety considerations during pregnancy. A provider should evaluate your individual situation before prescribing. Discuss your pregnancy status at your visit so treatment choices are appropriate.








